
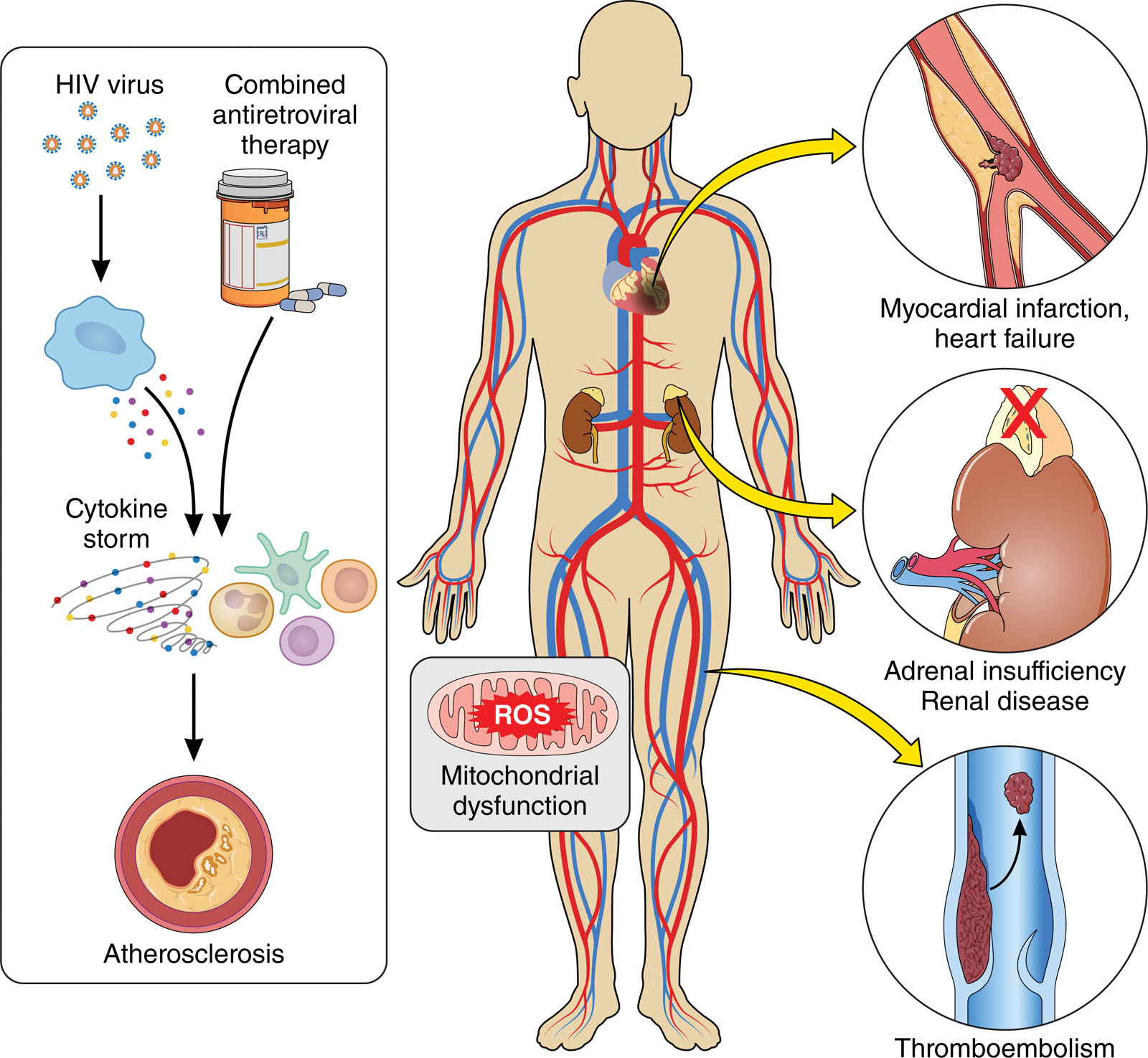
A growing body of research from Meharry Medical College in Nashville, Tennessee, the United States, is transforming the global understanding of HIV by uncovering its deep and long-underestimated relationship with cardiovascular disease.
Q1. Why is it important to look beyond HIV itself when discussing patients’ health today?
Dr. Gehad Elkady: It is important to look beyond HIV itself because the virus is associated with a wide range of serious diseases, such as; cardiovascular disease, increased risk of cancer, COVID-19, Hepatitis B, Hepatitis C, Human Papilloma, Kidney disease, as well as Tuberculosis (TB). Above all, persistent low-grade inflammation may continue even after the elimination of the virus reservoir.
Q2. Is it accurate to say that HIV is no longer the leading cause of death for many patients, but rather the complications associated with it?
Dr. Gehad Elkady: It may not be entirely accurate. However, HIV Elite controllers (ECs) are a rare group of people living with HIV, representing less than 1% of the infected population, who maintain undetectable viral loads and normal CD4 counts for years without antiviral therapy (ART).
They naturally control HIV-1 replication, often through robust immune responses—notably CD8+ T cells—and favorable genetic factors such as HLA-B57. These individuals with undetectable HIV RNA (usually ˂50 or ˂75 copies/ml) on standard tests while off ART.
Their bodies efficiently manage HIV-1, likely due to enhanced T-cell activity that keeps the virus in a state of “deep latency” often with viruses integrated into inactive areas of the genome. Even in ECs, however, chronic complications and comorbidities persist, including cardiovascular disease, an increased risk of cancer, and persistent low-grade inflammation.

Q3: The research highlights chronic inflammation as a major driver-why is this process so dangerous over time?
Dr. Gehad Elkady: Not only the non-progressive, low progressive, and high-progressive HIV groups, but also elite controllers, are vulnerable to chronic inflammation. Despite having low viral loads, they may still experience persistent inflammation and a higher risk of cardiovascular diseases, leading to discussions about whether they should receive treatment.
Therefore, studying these factors is crucial for developing HIV cures, therapeutic vaccines, and understanding how to achieve functional cures. However, challenges remain, particularly in treating solid tumors, where the immunosuppressive nature of tumor microenvironment can hinder CART cell efficacy.
Q4: The global burden of disease study shows a sharp rise in cardiovascular-related DALYs -what surprised you most in that data?
Dr. Gehad Elkady: People living with HIV (PLWH) face a higher risk of cardiovascular disease (CVD) than individuals without HIV.
Q5: Why are people in African countries more vulnerable to the combination of HIV and cardiovascular disease?
Dr. Gehad Elkady: The unhealthy lifestyle prevalent in developing regions is considered a major contributing factor, including low levels of physical activities and increased intake of high-calorie foods without adequate awareness. In addition, there is limited access to antiretroviral therapy (ART).
Q6: What are the most overlooked health risks facing people living with HIV worldwide today?
Dr. Gehad Elkady: For example, in elite controllers: Despite the absence of high-level viremia in some cases, they are not cured and face significant long-term health challenges. Some of these include:
- Cardiovascular disease (CVD): Elite controllers have a higher burden of subclinical atherosclerosis, coronary plaque, and carotid intima-media thickness compared to HIV-negative individuals.
- High hospitalization rates: One study found that elite controllers were hospitalized more frequently than patients with medically controlled HIV, particularly for cardiovascular and psychiatric reasons.
- Inflammatory Markers: Elite controllers show elevated levels of inflammatory markers (e.g.: sCD163, D-dimer) even when not on therapy.
- Clinical progression was often overlooked: Elite controllers experienced slow CD4+ T cell decline, loss of viral control (transient controllers), and AIDS-defining conditions.
- Chronic inflammation after ART: Not only the non-progressive, low progressive, and high-progressive HIV groups, but also elite controllers are vulnerable to chronic inflammation after receiving the ART.
Antiretroviral therapy (ART) such as latency reversing agents (LRAs) used to “shock” the system, is non-specific, leading to the activation of both infected and non-infected T-cells, which can contribute to chronic immune activation and systemic toxicity.
Q7: In your opinion, what are the most important unanswered questions that still require further research?
Dr. Gehad Elkady: The question is: what cutting-edge technology is currently used in HIV treatment?
Despite the benefits of ART therapy in improving the quality of life for HIV+ individuals, there are various risks and significant side effects associated with this combination of treatment.
Therefore, advancing the discovery of alternative therapeutic agents or effective vaccines is essential for HIV-1-infected individuals. For example:
1. Cell therapy:
Given HIV’s propensity to evade the natural immune response, early studies suggest that engineered T cells with improved recognition, persistence and efficacy are required to eradicate HIV.
This composite protein redirects T cells to a new target and endows them with effector functions upon antigen recognition, without the need for MHC presentation or co-receptor binding.
Moreover, additional cargo such as cytokines, chemokines, and cell surface markers can be engineered to co-express with the chimeric antigen receptors (CARs), augmenting the persistence, trafficking, and function of the CAR T cells.
Ongoing efforts to safely expand and engineer immune cells in an affordable manner may make cellular therapy a very attractive option for HIV treatment.
2. Exosome:
Some molecules such as proteins, nucleic acid-related signal transducers, lipids, membrane trafficking, T-cell stimulators, and anti-apoptotic particles present on the surface of exosomes have shown immune regulatory functions.
As biological nanovesicles with a poor immunogenic profile, exosomes hold high potential for the development of new vaccines based on nanoparticles.
By transmitting an inactive or natural adjuvant of antigens and virus particles, vaccines can result in a strong immune response.
To induce long-term, persistent epigenetic suppression of HIV-1, an approach was developed involving the creation of an HIV-1 promoter-targeting Zinc Finger Protein (ZFP-362) fused with the active domains of DNA methyltransferase 3A.
Cells were genetically modified to package exosomes containing RNAs encoding this HIV-1 repressor protein. Another study showed that exosomes produced from CD8+ T cells non-cytotoxically decrease HIV replication by inhibiting HIV-1 LTR promoter transcription.
Related Topics:
New Research Uncovers HIV–Heart Disease Connection
Saudi Health Ministry Addresses Concerns Over X Disease
WHO Declares Ebola Emergency: Congo, Uganda Outbreak Raises Global Alarm



